Pathology Case of the Month
May 08, 2017
Here in Disease Investigations we have a dedicated team of pathologists and technicians that have seen and performed hundreds to thousands of necropsies (animal autopsies) in our careers. Sometimes we feel that we must have seen it all, but then we get a case that reminds us there is always more to learn!
Such a case came to us recently. It was a baby Uganda kob, a type of African antelope, that was unable to keep up with its mother and could not be saved despite intervention by the dedicated veterinary team at the Safari Park. In Disease Investigations, we necropsy all animals that die at San Diego Zoo facilities to determine the cause of death and identify any disease conditions they might have. While we are most concerned about diseases with implications for the herd or group, we also find conditions that are simply nature’s bad luck. In the case of our kob, it was a congenital heart defect. Most of the time, these are a developmental anomaly, sporadic and unable to be explained. There are many different kinds of congenital heart defects, but this one was unlike any we had seen before.
You are probably aware that mammals have a four-chambered heart with two atria and two ventricles. Each side of the heart (right and left) has an atrium and a ventricle. Blood pumped from the left ventricle exits the heart via the aorta and travels to the whole body except the lungs. That blood returns to the right atrium and passes into the right ventricle, which then pumps blood to the lungs. Oxygenated blood returns from the lungs to the left atrium, which leads into the left ventricle, completing the path of circulation.
So what was so unusual about the heart from the kob? (See photos below in slide show.)
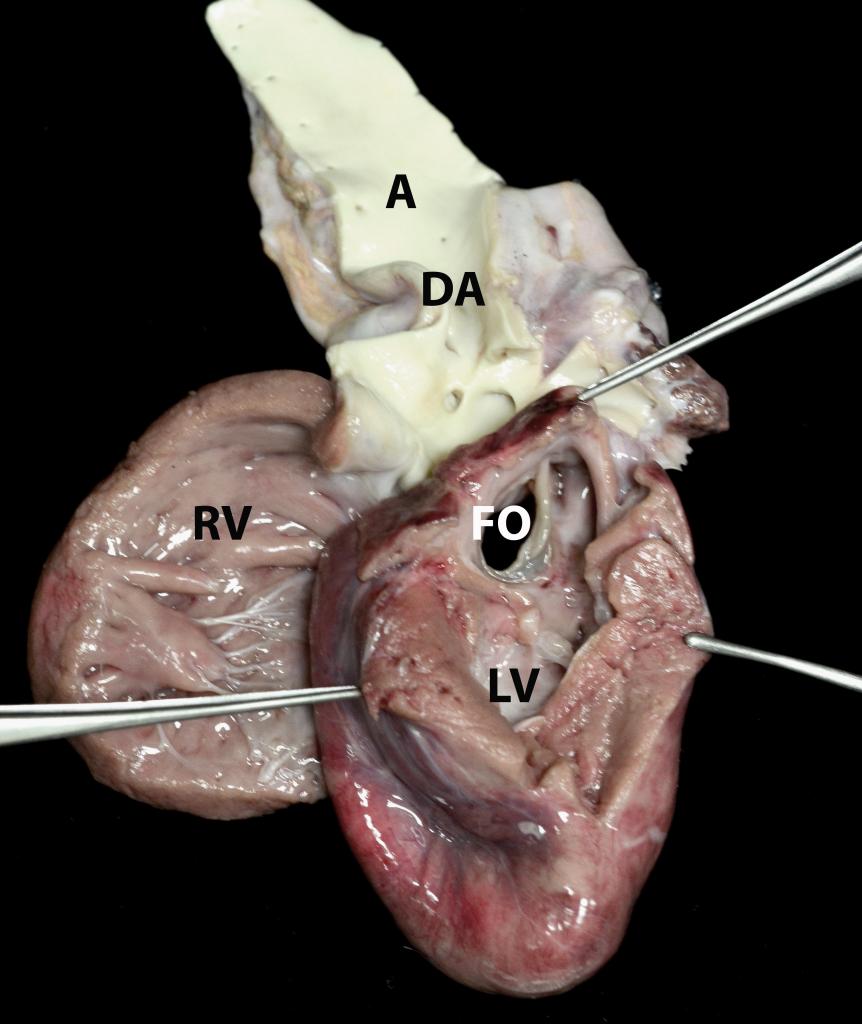
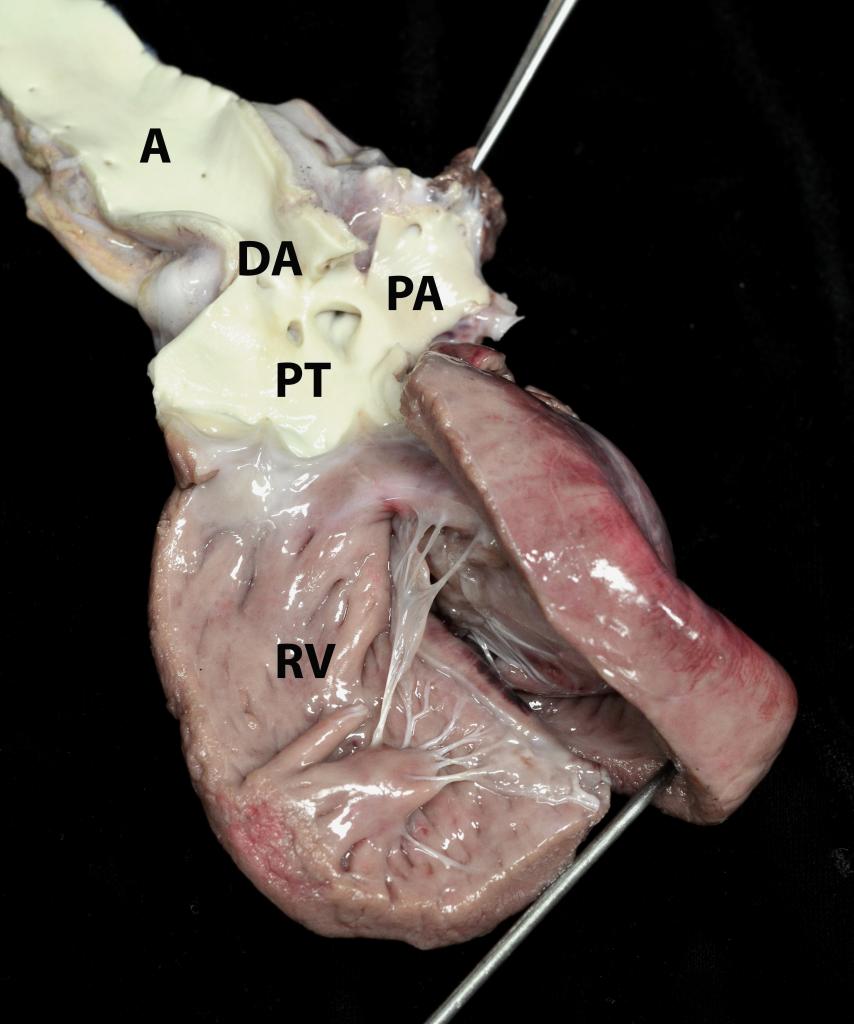
On the left side of the heart, the chambers, especially the left ventricle (LV), are much smaller than they should be (under-developed or hypoplastic), and there is no outflow tract from the left ventricle! The hole you see on this side (FO) is in the left atrium. Therefore blood could not get from the left ventricle into the aorta, which is the major artery that supplies blood to the whole body. On the right side, notice how much bigger the opened right ventricle (RV) is compared to the LV. It is abnormally dilated, and its outflow tract can be followed into the pulmonic trunk (PT), which leads into the pulmonary arteries (PA) as well as a large connection (DA) to the aorta (A). Note that there is no continuation of the aorta past this connection toward the left heart. It is hard to see how this defect was not immediately fatal!
The solution to the mystery lies in connections between the right and left heart and between the pulmonic trunk and the aorta that are open during fetal development. Blood circulates differently in the fetus because it is oxygenated by the placenta via the umbilical vessels and not by the lungs. The connections, one between the atria called the foramen ovale (FO) and one between the pulmonic trunk and the aorta called the ductus arteriosus (DA), normally close shortly after birth. In this case they remained open and allowed this kob to live, however briefly. In the images, the hole on the left side is the open foramen ovale between the left and right atrium. The aorta is connected to the pulmonic trunk at the site of the ductus arteriosus. We presume that blood was returning normally to the left heart but then passing directly into the right heart via the foramen ovale. Then the right ventricle was doing double the work in pumping blood to the lungs and the rest of body through the aorta’s connection to the pulmonic trunk. No wonder the right ventricle is so large!
This heart defect is so rare that it may be completely unique. We’re thinking of calling it the Burns-Takahashi malformation, since “aortic valve and ascending aorta atresia with left ventricular hypoplasia, patent ductus arteriosus and patent foramen ovale” is a little long.
Until the next weird one!